What Is Pain At The Heel

Overview
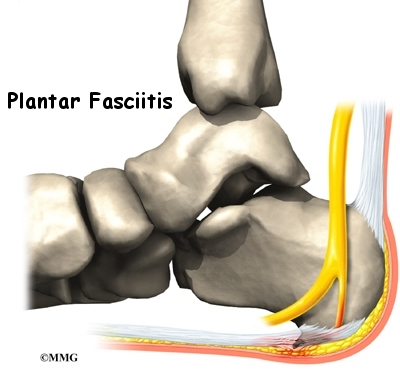
Plantar Fasciitis is a chronic pain in the heel that can just appear from nowhere but it is actually a long standing mechanical condition caused by prolonged stress on your foot. In most cases Plantar Fasciitis is a common, but very treatable, mechanical condition of the foot and responds positively to orthotics. A heel pain caused by prolonged stress on a ligament like structure in the arch that is very important in weigh-bearing activities. The tissue becomes damaged and needs to be helped to repair in order for the pain to go or subside to a manageable level. Orthotics for your feet can achieve this necessary healing for pain relief. It can be very painful, and even debilitating for sufferers.
Causes
Plantar fasciitis occurs when the thick band of tissue on the bottom of the foot is overstretched or overused. This can be painful and make walking more difficult. You are more likely to get plantar fasciitis if you Have foot arch problems (both flat feet and high arches), run long distances, downhill or on uneven surfaces, are obese or gain weight suddenly, have a tight Achilles tendon (the tendon connecting the calf muscles to the heel), wear shoes with poor arch support or soft soles. Plantar fasciitis is seen in both men and women. However, it most often affects active men ages 40 - 70. It is one of the most common orthopedic foot complaints. Plantar fasciitis was commonly thought to be caused by a heel spur. However, research has found that this is not the case. On x-ray, heel spurs are seen in people with and without plantar fasciitis.
Symptoms
Symptoms of the plantar fasciitis include a gradual onset of pain under the heel which may radiate into the foot. Tenderness is usually felt under and on the inside of the heel which is initially worse first in the morning but eases as the foot warms up only to return later in the day or after exercise. Stretching the plantar fascia may be painful.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
A steroid (cortisone) injection is sometimes tried if your pain remains bad despite the above 'conservative' measures. It may relieve the pain in some people for several weeks but does not always cure the problem. It is not always successful and may be sore to have done. Steroids work by reducing inflammation. Sometimes two or three injections are tried over a period of weeks if the first is not successful. Steroid injections do carry some risks, including (rarely) tearing (rupture) of the plantar fascia. Extracorporeal shock-wave therapy. In extracorporeal shock-wave therapy, a machine is used to deliver high-energy sound waves through your skin to the painful area on your foot. It is not known exactly how it works, but it is thought that it might stimulate healing of your plantar fascia. One or more sessions of treatment may be needed. This procedure appears to be safe but it is uncertain how well it works. This is mostly because of a lack of large, well-designed clinical trials. You should have a full discussion with your doctor about the potential benefits and risks. In studies, most people who have had extracorporeal shock-wave therapy have little in the way of problems. However, possible problems that can occur include pain during treatment, skin reddening, and swelling of your foot or bruising. Another theoretical problem could include the condition getting worse because of rupture of your plantar fascia or damage to the tissues in your foot. More research into extracorporeal shock-wave therapy for plantar fasciitis is needed. Other treatments. Various studies and trials have been carried out looking at other possible treatments for plantar fasciitis. Such treatments include injection with botulinum toxin and treatment of the plantar fascia with radiotherapy. These treatments may not be widely available. Some people benefit from wearing a special splint overnight to keep their Achilles tendon and plantar fascia slightly stretched. The aim is to prevent the plantar fascia from tightening up overnight. In very difficult cases, sometimes a plaster cast or a removable walking brace is put on the lower leg. This provides rest, protection, cushioning and slight stretching of the plantar fascia and Achilles tendon. However, the evidence for the use of splint treatment of plantar fasciitis is limited.
Surgical Treatment
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.