Contracted Toe Medical Operation
 Overview
Overview
Hammer toe is a Z-shaped deformity caused by dorsal subluxation at the metatarsophalangeal joint. Diagnosis is clinical. Treatment is modification of footwear and/or orthotics. The usual cause is misalignment of the joint surfaces due to a genetic predisposition toward aberrant foot biomechanics and tendon contractures. RA and neurologic disorders such as Charcot-Marie-Tooth disease are other causes.
Causes
As described hammertoe above, the main reason people develop hammertoes is improper footwear, or footwear that is too short for the toes. Shoes that do not allow our toes to lie flat are the biggest cause of hammertoes, though there are others, including genetics, injury or trauma in which the toe is jammed or broken. Diseases that affect the nerves and muscles, such as arthritis. Abnormal foot mechanics due to nerve or muscle damage, causing an imbalance of the flexor and extensor tendons of the toe. Systematic diseases such as arthritis can also lead to problems such as hammertoe. Some people are born with hammertoes, while others are more prone to developing the condition due to genetics. If you have ever broken a toe, you know there is not much that can be done for it. It is one of the only bones in the body that heals without the use of a cast. A broken toe may be splinted, however, which may help prevent a hammertoe from forming.
 Symptoms
Symptoms
A soft corn, or heloma molle, may exist in the web space between toes. This is more commonly caused by an exostosis, which is basically an extra growth of bone possibly due to your foot structure. As this outgrowth of excessive bone rubs against other toes, there is friction between the toes and a corn forms for your protection.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
The most common treatment is to wear more comfortable shoes. When choosing a shoe, make sure the toe area is high and broad and has enough room for hammer toes. If there is chronic pain, surgery may be needed to correct a malalignment. Surgical treatments are aimed at loosening up the contracted toe joints to allow them to align properly. Other types of treatment are products designed to relieve hammer toes, such as hammer toe crests and hammer toe splints. These devices will help hold down the hammer toe and provide relief to the forefoot. Gel toe shields and gel toe caps can also be used. Gel toe shields and toe caps will help eliminate friction between the shoe and the toe, while providing comfort and lubrication.
Surgical Treatment
Surgically correcting a hammertoe is very technical and difficult, and requires a surgeon with superior capabilities and experience. The operation can be done at our office or the hospital with local anesthetic. After making a small incision, the deformity is reduced and the tendons are realigned at the joint. You will be able to go home the same day with a special shoe! If you are sick and tired of not fitting your shoes, you can no longer get relief from pads, orthopedic shoes or pedicures, and have corns that are ugly, sensitive and painful, then you certainly may be a good surgical candidate. In order to have this surgery, you can not have poor circulation and and must have a clean bill of health.
Hallux Abducto Valgus Treatment
Overview
 More than one-third of women in America have bunions, a common deformity often blamed on wearing tight, narrow shoes and high heels. Bunions may occur in families, but many are from wearing tight shoes, and nine out of 10 bunions happen to women. Too-tight shoes can also cause other disabling foot problems such as corns, calluses and hammer toes.
More than one-third of women in America have bunions, a common deformity often blamed on wearing tight, narrow shoes and high heels. Bunions may occur in families, but many are from wearing tight shoes, and nine out of 10 bunions happen to women. Too-tight shoes can also cause other disabling foot problems such as corns, calluses and hammer toes.
Causes
Foot problems typically develop in early adulthood and get worse as the foot spreads with aging. For many people, bunions run in the family. They may be just one of several problems due to weak or poor foot structure. Bunions sometimes develop with arthritis. In people with leg length discrepancies, bunions usually form in the longer leg. Women are especially prone to developing bunions. Years of wearing tight, poorly fitting shoes especially high-heeled, pointed shoes can bring on bunions. Such shoes gradually push the foot bones into an unnatural shape.
Symptoms
Symptoms, which occur at the site of the bunion, may include pain or soreness, inflammation and redness, a burning sensation, possible numbness. Symptoms occur most often when wearing shoes that crowd the toes, such as shoes with a tight toe box or high heels. This may explain why women are more likely to have symptoms than men. In addition, spending long periods of time on your feet can aggravate the symptoms of bunions.
Diagnosis
Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly.
Non Surgical Treatment
Bunions may be treated with proper shoes and corrective inserts such as toe spacers, bunion or toe separators, as well as bunion cushions and splints. In extreme cases, surgery may be needed to remove the bony enlargement of the first metatarsal bone, realigning the bone, or straightening the big toe. 
Surgical Treatment
Surgery is the only way to correct a bunion. A bunion will usually get worse over time, so if it's left untreated it's likely to get bigger and become more painful. If your bunion is causing a significant amount of pain and affecting your quality of life, your GP may refer you to be assessed for bunion surgery. The aim of surgery is to relieve pain and improve the alignment of your big toe. Surgery isn't usually carried out for cosmetic reasons alone. Even after surgery, there may still be limits to the styles of shoe you can wear. Bunion surgery is often carried out as a day procedure, which means you won't have to stay in hospital overnight. The procedure will either be carried out under a local anaesthetic or a general anaesthetic.
Prevention
To help prevent bunions, select your style and size of shoes wisely. Choose shoes with a wide toe area and a half-inch of space between the tip of your longest toe and the end of the shoe. Shoes also should conform to the shape of your feet without causing too much pressure.
Do You Know The Chief Causes Of Over-Pronation Of The Foot
Overview
One of the most common causes of foot and leg discomfort is a condition known as overpronation. Normal pronation, or "turning inward" of the foot is necessary as the foot adapts to the ground. With over pronation, the arch flattens, collapses, and soft tissues stretch. This causes the joint surfaces to function at unnatural angles to each other. When this happens, joints that should be stable now become very loose and flexible. At first, over pronation may cause fatigue. As the problem gets worse, strain on the muscles, tendons, and ligaments of the foot and lower leg can cause permanent problems and deformities.
Causes
There are many possible causes for overpronation, but researchers have not yet determined one underlying cause. Hintermann states, Compensatory overpronation may occur for anatomical reasons, such as a tibia vara of 10 degrees or more, forefoot varus, leg length discrepancy, ligamentous laxity, or because of muscular weakness or tightness in the gastrocnemius and soleus muscles. Pronation can be influenced by sources outside of the body as well. Shoes have been shown to significantly influence pronation. Hintermann states that the same person can have different amounts of pronation just by using different running shoes. It is easily possible that the maximal ankle joint eversion movement is 31 degrees for one and 12 degrees for another running shoe.
Symptoms
When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Get a gait analysis of your running style, this will highlight if you overpronate, oversupinate or have a neutral gait. Most podiatrists, physio's and sports therapists will offer this service, as do some specialist sports shops. Find a clinic. If you overpronate, get orthotics with extra medial support. Many running shoes have a harder material on the inside of the midsole (the thick hard foam part of the running shoe). This means the inside of the shoe will be compressed less under load and support the inside of the foot preventing it from rolling in or flattening. For people with considerable overpronation, another option is to have an orthotic device fitted. Orthotic insoles come in many types and prices. Some are pre-molded and can be bought off the shelf. These are ok for the majority of problem feet. However some cases may require specially casted orthotics from a relevant sports injury therapist or podiatrist.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
One of the most common causes of foot and leg discomfort is a condition known as overpronation. Normal pronation, or "turning inward" of the foot is necessary as the foot adapts to the ground. With over pronation, the arch flattens, collapses, and soft tissues stretch. This causes the joint surfaces to function at unnatural angles to each other. When this happens, joints that should be stable now become very loose and flexible. At first, over pronation may cause fatigue. As the problem gets worse, strain on the muscles, tendons, and ligaments of the foot and lower leg can cause permanent problems and deformities.
Causes
There are many possible causes for overpronation, but researchers have not yet determined one underlying cause. Hintermann states, Compensatory overpronation may occur for anatomical reasons, such as a tibia vara of 10 degrees or more, forefoot varus, leg length discrepancy, ligamentous laxity, or because of muscular weakness or tightness in the gastrocnemius and soleus muscles. Pronation can be influenced by sources outside of the body as well. Shoes have been shown to significantly influence pronation. Hintermann states that the same person can have different amounts of pronation just by using different running shoes. It is easily possible that the maximal ankle joint eversion movement is 31 degrees for one and 12 degrees for another running shoe.
Symptoms
When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Get a gait analysis of your running style, this will highlight if you overpronate, oversupinate or have a neutral gait. Most podiatrists, physio's and sports therapists will offer this service, as do some specialist sports shops. Find a clinic. If you overpronate, get orthotics with extra medial support. Many running shoes have a harder material on the inside of the midsole (the thick hard foam part of the running shoe). This means the inside of the shoe will be compressed less under load and support the inside of the foot preventing it from rolling in or flattening. For people with considerable overpronation, another option is to have an orthotic device fitted. Orthotic insoles come in many types and prices. Some are pre-molded and can be bought off the shelf. These are ok for the majority of problem feet. However some cases may require specially casted orthotics from a relevant sports injury therapist or podiatrist.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
The Way To Spot Calcaneal Apophysitis?
Overview
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
One of the most common causes of heel pain in adolescents, Sever's disease is an overuse injury to the growth plate of the calcaneus (heel). It is commonly seen in growing, active children 8-12 years of age. Soccer players, gymnasts, and children who do any sort of running or jumping activity have an increased risk of developing Sever's disease. Occurring in one or both feet, Sever?s disease occurs at the back of the heel (also known as the apophysis or the insertion of the Achilles tendon).
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Treatment is primarily supportive, with rest, pain management, and activity modification. Activity modifications include the addition of low-impact activities. Gel heel cups are sold over the counter and can be used intermittently to help reduce shock in the heel, as well as take tension off of the tight Achilles?s tendon complex. Proper stretching and strengthening activities should be preformed routinely even during periods of no pain. A large study showed that approximately 85% of children affected by Sever?s disease return to full activity within a two-month time period after starting treatment.
Recovery
One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away. Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
One of the most common causes of heel pain in adolescents, Sever's disease is an overuse injury to the growth plate of the calcaneus (heel). It is commonly seen in growing, active children 8-12 years of age. Soccer players, gymnasts, and children who do any sort of running or jumping activity have an increased risk of developing Sever's disease. Occurring in one or both feet, Sever?s disease occurs at the back of the heel (also known as the apophysis or the insertion of the Achilles tendon).
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
To diagnose the cause of the child?s heel pain and rule out other more serious conditions, the foot and ankle surgeon obtains a thorough medical history and asks questions about recent activities. The surgeon will also examine the child?s foot and leg. X-rays are often used to evaluate the condition. Other advanced imaging studies and laboratory tests may also be ordered.
Non Surgical Treatment
Treatment is primarily supportive, with rest, pain management, and activity modification. Activity modifications include the addition of low-impact activities. Gel heel cups are sold over the counter and can be used intermittently to help reduce shock in the heel, as well as take tension off of the tight Achilles?s tendon complex. Proper stretching and strengthening activities should be preformed routinely even during periods of no pain. A large study showed that approximately 85% of children affected by Sever?s disease return to full activity within a two-month time period after starting treatment.
Recovery
One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away. Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
Will Adult Aquired FlatFoot Call For Surgical Pocedures ?
Overview
Adult acquired flatfoot deformity, primarily posterior tibial tendon dysfunction, in many cases can be successfully managed with conservative treatment modalities including early immobilization, long-term bracing, physi?cal therapy, and anti-inflam?matory medications. Adult acquired flatfoot deformity (AAFD), the painful flatfoot deformity in adults, is a major cause of disability for a patient and can be a challenge for foot and ankle specialists. 
Causes
There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction.
Symptoms
Symptoms of pain may have developed gradually as result of overuse or they may be traced to one minor injury. Typically, the pain localizes to the inside (medial) aspect of the ankle, under the medial malleolus. However, some patients will also experience pain over the outside (lateral) aspect of the hindfoot because of the displacement of the calcaneus impinging with the lateral malleolus. This usually occurs later in the course of the condition. Patients may walk with a limp or in advanced cases be disabled due to pain. They may also have noticed worsening of their flatfoot deformity.
Diagnosis
Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot.
Non surgical Treatment
Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found. 
Surgical Treatment
If conservative treatment fails surgical intervention is offered. For a Stage 1 deformity a posterior tibial tendon tenosynovectomy (debridement of the tendon) or primary repair may be indicated. For Stage 2 a combination of Achilles lengthening with bone cuts, calcaneal osteotomies, and tendon transfers is common. Stage 2 flexible PTTD is the most common stage patients present with for treatment. In Stage 3 or 4 PTTD isolated fusions, locking two or more joints together, maybe indicated. All treatment is dependent on the stage and severity at presentation with the goals and activity levels of the patient in mind. Treatment is customized to the individual patient needs.
What Causes Heel Serious Pain
Overview

Heel pain is a very common foot complaint and may involve injury to the bone, fat pad, ligaments, tendons or muscles. Heel Pain can also be referred by a pinched nerve in your lower back. It is important to have your heel pain thoroughly assessed to ensure an accurate diagnosis and subsequent treatment. Anyone can suffer from heel pain, but certain groups seem to be at increased risk, including middle aged men and women, active people eg running sports, people who are very overweight, children aged between 8 and 13 years, pregnant women, people who stand for long periods of time.
Causes
There is no one cause of heel pain. Whole text books have been written on Disorders of the Heel. Some of the types of problems that can be seen in the heel include Heel spurs, these are small bony spurs that often develop on the bottom of the heel. They do not really cause any problems. It is only mentioned here as it is a common myth that they are a problem - almost always the pain associated with heel spurs is really plantar fasciitis. Plantar fasciitis is the most common cause of heel pain and is due to a strain of the long ligament along the bottom of the foot. The most symptom is pain when getting out of bed first thing in the morning ('post-static dyskinesia') A number of disease processes can uncommonly cause heel pain, such as rheumatoid arthritis, ankylosing spondylitis and gout. Stress fractures, which is an abnormal reaction of bone to stress can occur in those that are very active (eg athletes) or have weaker bones (eg osteoporosis) Pain at the back of the heel could be due to a number of problems, there could be a bursitis at the back of the heel bone (sometimes called 'Haglund's) there could be problems with the insertion of the achilles tendon, such as tendonitis or calcification. A 'stone' bruise is sometimes considered to be a cause of heel pain, its is simply a bruise of the bone. Another cause of heel pain is problems in the calf muscles that refer pain to the heel (myofascial trigger points) or pain referred from the lower back via the nerves from the back to the heel. Heel pain in children is usually due to severs disease or calcaneal apophysitis.
Symptoms
The primary symptom is pain in the heel area that varies in severity and location. The pain is commonly intense when getting out of bed or a chair. The pain often lessens when walking.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
Shoes, orthoses, splinting and/or immobilization form the cornerstone for successful functional management of plantar fasciitis.When you take the overuse nature of plantar fasciitis into account and attempt to re-establish the windlass mechanism of the foot, there is an enhanced potential for success. Unfortunately, too little attention has been directed to appropriately managing the shoes worn during treatment for plantar fasciitis. Emphasising motion control and stability type athletic shoes (that provide a firm heel cup, instep rigidity, longitudinal integrity and a well-integrated shoe upper) can help decrease excess eccentric tissue strain. The shoe also serves as a vital and functional link between an orthotic and the foot. Orthoses have long been considered to be a reliable method for treating plantar fasciitis. Considerable debate has been waged over the benefits of over-the-counter (OTC), prefabricated and prescription foot and/or ankle orthoses. Heel cushions, heel cups and cushioning pads appear to provide immediate pain relief for many people who have plantar fasciitis.This relief is frequently short-lived and requires other treatment modalities for success.Neutral position taping and strapping of the foot provides temporary symptomatic relief of pain caused by plantar fasciitis. Although the functional benefits are temporary and likely do not last longer than 10 minutes with exercise, the soft tissue compression and symptomatic relief afforded by the strapping can last for nearly a week.
Surgical Treatment
It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation.
Prevention

Preventing heel pain is crucial to avoid pain that can easily interrupt a busy or active lifestyle. Athletes can prevent damage by stretching the foot and calf both before and after an exercise routine. The plantar fascia ligament can be stretched by using a tennis ball or water bottle and rolling it across the bottom of the foot. With regular stretching, the stretching and flexibility of tissue through the foot can be significantly improved, helping to prevent damage and injury. Athletes should also ease into new or more difficult routines, allowing the plantar fascia and other tissue to become accustomed to the added stress and difficulty. Running up hills is also common among athletes in their routines. However, this activity should be reduced since it places an increased amount of stress on the plantar fascia and increases the risk of plantar fasciitis. Maintaining a healthy weight is also an essential heel pain prevention technique. Obesity brings additional weight and stress on the heel of the foot, causing damage and pain in the heel as well as in other areas of the foot.
Heel pain is a very common foot complaint and may involve injury to the bone, fat pad, ligaments, tendons or muscles. Heel Pain can also be referred by a pinched nerve in your lower back. It is important to have your heel pain thoroughly assessed to ensure an accurate diagnosis and subsequent treatment. Anyone can suffer from heel pain, but certain groups seem to be at increased risk, including middle aged men and women, active people eg running sports, people who are very overweight, children aged between 8 and 13 years, pregnant women, people who stand for long periods of time.
Causes
There is no one cause of heel pain. Whole text books have been written on Disorders of the Heel. Some of the types of problems that can be seen in the heel include Heel spurs, these are small bony spurs that often develop on the bottom of the heel. They do not really cause any problems. It is only mentioned here as it is a common myth that they are a problem - almost always the pain associated with heel spurs is really plantar fasciitis. Plantar fasciitis is the most common cause of heel pain and is due to a strain of the long ligament along the bottom of the foot. The most symptom is pain when getting out of bed first thing in the morning ('post-static dyskinesia') A number of disease processes can uncommonly cause heel pain, such as rheumatoid arthritis, ankylosing spondylitis and gout. Stress fractures, which is an abnormal reaction of bone to stress can occur in those that are very active (eg athletes) or have weaker bones (eg osteoporosis) Pain at the back of the heel could be due to a number of problems, there could be a bursitis at the back of the heel bone (sometimes called 'Haglund's) there could be problems with the insertion of the achilles tendon, such as tendonitis or calcification. A 'stone' bruise is sometimes considered to be a cause of heel pain, its is simply a bruise of the bone. Another cause of heel pain is problems in the calf muscles that refer pain to the heel (myofascial trigger points) or pain referred from the lower back via the nerves from the back to the heel. Heel pain in children is usually due to severs disease or calcaneal apophysitis.
Symptoms
The primary symptom is pain in the heel area that varies in severity and location. The pain is commonly intense when getting out of bed or a chair. The pain often lessens when walking.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
Shoes, orthoses, splinting and/or immobilization form the cornerstone for successful functional management of plantar fasciitis.When you take the overuse nature of plantar fasciitis into account and attempt to re-establish the windlass mechanism of the foot, there is an enhanced potential for success. Unfortunately, too little attention has been directed to appropriately managing the shoes worn during treatment for plantar fasciitis. Emphasising motion control and stability type athletic shoes (that provide a firm heel cup, instep rigidity, longitudinal integrity and a well-integrated shoe upper) can help decrease excess eccentric tissue strain. The shoe also serves as a vital and functional link between an orthotic and the foot. Orthoses have long been considered to be a reliable method for treating plantar fasciitis. Considerable debate has been waged over the benefits of over-the-counter (OTC), prefabricated and prescription foot and/or ankle orthoses. Heel cushions, heel cups and cushioning pads appear to provide immediate pain relief for many people who have plantar fasciitis.This relief is frequently short-lived and requires other treatment modalities for success.Neutral position taping and strapping of the foot provides temporary symptomatic relief of pain caused by plantar fasciitis. Although the functional benefits are temporary and likely do not last longer than 10 minutes with exercise, the soft tissue compression and symptomatic relief afforded by the strapping can last for nearly a week.
Surgical Treatment
It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation.
Prevention
Preventing heel pain is crucial to avoid pain that can easily interrupt a busy or active lifestyle. Athletes can prevent damage by stretching the foot and calf both before and after an exercise routine. The plantar fascia ligament can be stretched by using a tennis ball or water bottle and rolling it across the bottom of the foot. With regular stretching, the stretching and flexibility of tissue through the foot can be significantly improved, helping to prevent damage and injury. Athletes should also ease into new or more difficult routines, allowing the plantar fascia and other tissue to become accustomed to the added stress and difficulty. Running up hills is also common among athletes in their routines. However, this activity should be reduced since it places an increased amount of stress on the plantar fascia and increases the risk of plantar fasciitis. Maintaining a healthy weight is also an essential heel pain prevention technique. Obesity brings additional weight and stress on the heel of the foot, causing damage and pain in the heel as well as in other areas of the foot.
The Causes And Treatment Of Achilles Tendon Pain
Overview
 Achilles tendinitis is one of the more common causes of heel pain and many people describe it as pain in the back of the heel. Since this condition is a form of tendinitis, patients mostly notice that the back of their heel is inflamed. The Achilles tendon is the largest tendon in your body. It is also one of the most important and most used parts of the body. It is essential for walking, running, jumping or even just an extension of the foot. It is for this reason that Achilles tendinitis can affect anyone who is constantly putting stress on his or her foot. Athletes are particularly at risk.
Achilles tendinitis is one of the more common causes of heel pain and many people describe it as pain in the back of the heel. Since this condition is a form of tendinitis, patients mostly notice that the back of their heel is inflamed. The Achilles tendon is the largest tendon in your body. It is also one of the most important and most used parts of the body. It is essential for walking, running, jumping or even just an extension of the foot. It is for this reason that Achilles tendinitis can affect anyone who is constantly putting stress on his or her foot. Athletes are particularly at risk.
Causes
As ?overuse? disorders, Achilles tendonitis and tendonosis are usually caused by a sudden increase of a repetitive activity involving the Achilles tendon. Such activity puts too much stress on the tendon too quickly, leading to micro-injury of the tendon fibers. Due to this ongoing stress on the tendon, the body is unable to repair the injured tissue. The structure of the tendon is then altered, resulting in continued pain. Achilles4Athletes are at high risk for developing disorders of the Achilles tendon. Achilles tendonitis and tendonosis are also common in individuals whose work puts stress on their ankles and feet, such as laborers, as well as in ?weekend warriors?-those who are less conditioned and participate in athletics only on weekends or infrequently. In addition, people with excessive pronation (flattening of the arch) have a tendency to develop Achilles tendonitis and tendonosis due to the greater demands placed on the tendon when walking. If these individuals wear shoes without adequate stability, their over-pronation could further aggravate the Achilles tendon.
Symptoms
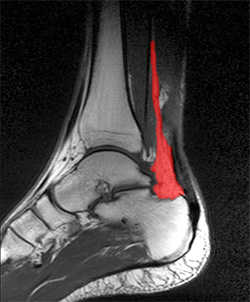
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
If Achilles tendonitis is suspected, avoid any exercise or activity that causes the pain. It is advisable to see a doctor promptly so that an accurate diagnosis can be made and appropriate treatment recommended. The doctor will take a full medical history and will ask about the nature and duration of the symptoms. They will perform a physical examination of the affected area. Ultrasound scanning may be used to assess damage to the tendon or surrounding structures. Occasionally MRI (magnetic resonance imaging) may be recommended. The symptoms of Achilles tendonitis are often similar to symptoms of other conditions such as partial Achilles tendon rupture and heel bursitis. This can make diagnosis difficult and a referral to an orthopaedic specialist may be required in order for an accurate diagnosis to be made.
Nonsurgical Treatment
As with most soft tissue injuries the initial treatment is RICE - Rest, Ice, Compression and Elevation. In the early phase you?ll be unable to walk without a limp, so your Achilles tendon needs some active rest from weight-bearing loads. You may need to be non or partial-weight-bearing, utilise crutches, a wedged achilles walking boot or heel wedges to temporarily relieve some of the pressure on the Achilles tendon. Your physiotherapist will advise you on what they feel is best for you. Ice is a simple and effective modality to reduce your pain and swelling. Please apply for 20-30 minutes each 2 to 4 hours during the initial phase or when you notice that your injury is warm or hot. Anti-inflammatory medication (if tolerated) and natural substances eg arnica may help reduce your pain and swelling. However, it is best to avoid anti-inflammatory drugs during the initial 48 to 72 hours when they may encourage additional bleeding. Most people can tolerate paracetamol as a pain reducing medication. As you improve a kinesio style supportive taping will help to both support the injured soft tissue.

Surgical Treatment
Surgery for an Achilles tendon rupture can be done with a single large incision, which is called open surgery. Or it can be done with several small incisions. This is called percutaneous surgery. The differences in age and activity levels of people who get surgery can make it hard to know if Achilles tendon surgery is effective. The success of your surgery can depend on, your surgeon's experience. The type of surgery you have. How damaged the tendon is. How soon after rupture the surgery is done. How soon you start your rehab program after surgery. How well you follow your rehab program. Talk to your surgeon about his or her surgical experience. Ask about his or her success rate with the technique that would best treat your condition.
Prevention
The following measures can significantly reduce the risk of developing Achilles tendonitis. Adequately stretch and warm up prior to exercise. Warm down and stretch after exercise. Choose footwear carefully and use footwear appropriate to the sport being undertaken. Use orthotic devices in footwear to correctly support the foot. Exercise within fitness levels and follow a sensible exercise programme. Develop strong, flexible calf muscles.
Achilles tendinitis is one of the more common causes of heel pain and many people describe it as pain in the back of the heel. Since this condition is a form of tendinitis, patients mostly notice that the back of their heel is inflamed. The Achilles tendon is the largest tendon in your body. It is also one of the most important and most used parts of the body. It is essential for walking, running, jumping or even just an extension of the foot. It is for this reason that Achilles tendinitis can affect anyone who is constantly putting stress on his or her foot. Athletes are particularly at risk.
Causes
As ?overuse? disorders, Achilles tendonitis and tendonosis are usually caused by a sudden increase of a repetitive activity involving the Achilles tendon. Such activity puts too much stress on the tendon too quickly, leading to micro-injury of the tendon fibers. Due to this ongoing stress on the tendon, the body is unable to repair the injured tissue. The structure of the tendon is then altered, resulting in continued pain. Achilles4Athletes are at high risk for developing disorders of the Achilles tendon. Achilles tendonitis and tendonosis are also common in individuals whose work puts stress on their ankles and feet, such as laborers, as well as in ?weekend warriors?-those who are less conditioned and participate in athletics only on weekends or infrequently. In addition, people with excessive pronation (flattening of the arch) have a tendency to develop Achilles tendonitis and tendonosis due to the greater demands placed on the tendon when walking. If these individuals wear shoes without adequate stability, their over-pronation could further aggravate the Achilles tendon.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
If Achilles tendonitis is suspected, avoid any exercise or activity that causes the pain. It is advisable to see a doctor promptly so that an accurate diagnosis can be made and appropriate treatment recommended. The doctor will take a full medical history and will ask about the nature and duration of the symptoms. They will perform a physical examination of the affected area. Ultrasound scanning may be used to assess damage to the tendon or surrounding structures. Occasionally MRI (magnetic resonance imaging) may be recommended. The symptoms of Achilles tendonitis are often similar to symptoms of other conditions such as partial Achilles tendon rupture and heel bursitis. This can make diagnosis difficult and a referral to an orthopaedic specialist may be required in order for an accurate diagnosis to be made.
Nonsurgical Treatment
As with most soft tissue injuries the initial treatment is RICE - Rest, Ice, Compression and Elevation. In the early phase you?ll be unable to walk without a limp, so your Achilles tendon needs some active rest from weight-bearing loads. You may need to be non or partial-weight-bearing, utilise crutches, a wedged achilles walking boot or heel wedges to temporarily relieve some of the pressure on the Achilles tendon. Your physiotherapist will advise you on what they feel is best for you. Ice is a simple and effective modality to reduce your pain and swelling. Please apply for 20-30 minutes each 2 to 4 hours during the initial phase or when you notice that your injury is warm or hot. Anti-inflammatory medication (if tolerated) and natural substances eg arnica may help reduce your pain and swelling. However, it is best to avoid anti-inflammatory drugs during the initial 48 to 72 hours when they may encourage additional bleeding. Most people can tolerate paracetamol as a pain reducing medication. As you improve a kinesio style supportive taping will help to both support the injured soft tissue.
Surgical Treatment
Surgery for an Achilles tendon rupture can be done with a single large incision, which is called open surgery. Or it can be done with several small incisions. This is called percutaneous surgery. The differences in age and activity levels of people who get surgery can make it hard to know if Achilles tendon surgery is effective. The success of your surgery can depend on, your surgeon's experience. The type of surgery you have. How damaged the tendon is. How soon after rupture the surgery is done. How soon you start your rehab program after surgery. How well you follow your rehab program. Talk to your surgeon about his or her surgical experience. Ask about his or her success rate with the technique that would best treat your condition.
Prevention
The following measures can significantly reduce the risk of developing Achilles tendonitis. Adequately stretch and warm up prior to exercise. Warm down and stretch after exercise. Choose footwear carefully and use footwear appropriate to the sport being undertaken. Use orthotic devices in footwear to correctly support the foot. Exercise within fitness levels and follow a sensible exercise programme. Develop strong, flexible calf muscles.